
Physiotherapists and Priority Setting: A Focus Group Study in Municipalities in Finnmark, Norway
Scientific article in Fysioterapeuten. The original version was published in Norwegian, Fysioterapeuten 1/2015.
Morten Nikolaisen, specialist in neurological physiotherapy (MNFF), MSc, PT, Department of Rehabilitation, Finnmark Hospital Trust (Kirkenes). morten@nikolaisen.me
Cathrine Arntzen, associate professor, ph.d., Department of Health and Care Sciences, UiT The Arctic University of Norway
Siri Moe, associate professor, dr. philos, Department of Health and Care Sciences, UiT The Arctic University of Norway
This scientific article is peer reviewed by the Fysioterapeuten’s guidelines, and was accepted 12.03.2014. Norwegian Social Science Data Services (NSD) approved this study. No conflicts of interest stated.
Abstract
Purpose: The article discusses how municipally employed physiotherapists and private practicing physiotherapists in Finnmark’s municipalities describe and reason about prioritization and allocation of tasks. The objective of the study was to gain more knowledge about content and tradeoffs in physiotherapy services and see if professional practice and development are in line with current health policies.
Method: The study is based on five focus group interviews with physiotherapists (n=21).
Findings: The participants perceived municipal resources for physiotherapy as insufficient, and expressed that they had to perform demanding prioritizations with limited support from the local authorities. Due to long distances to travel, patients who needed home consultations were in danger of not getting physiotherapy. Traditional differences between private practitioners and municipally employed physiotherapists characterized prioritization and distribution of patient groups and tasks. In municipalities with fewer physiotherapists and a wider range of tasks, the differences were less apparent. Municipally employed physiotherapists were given new tasks without an increase in capacity in the physiotherapy services, and distributed their resources on more patients than professionally desirable.
Conclusion: Limited service capacity, variations in affiliation (private practicing or municipally employed) and prioritizations, plus long distances, causes differences in provided physiotherapy services depending on place of residence. This emphasizes the importance of municipalities attending to their overall responsibility for physiotherapy services.
Key words: physiotherapy, primary health care, rural health services, health priorities.
Introduction
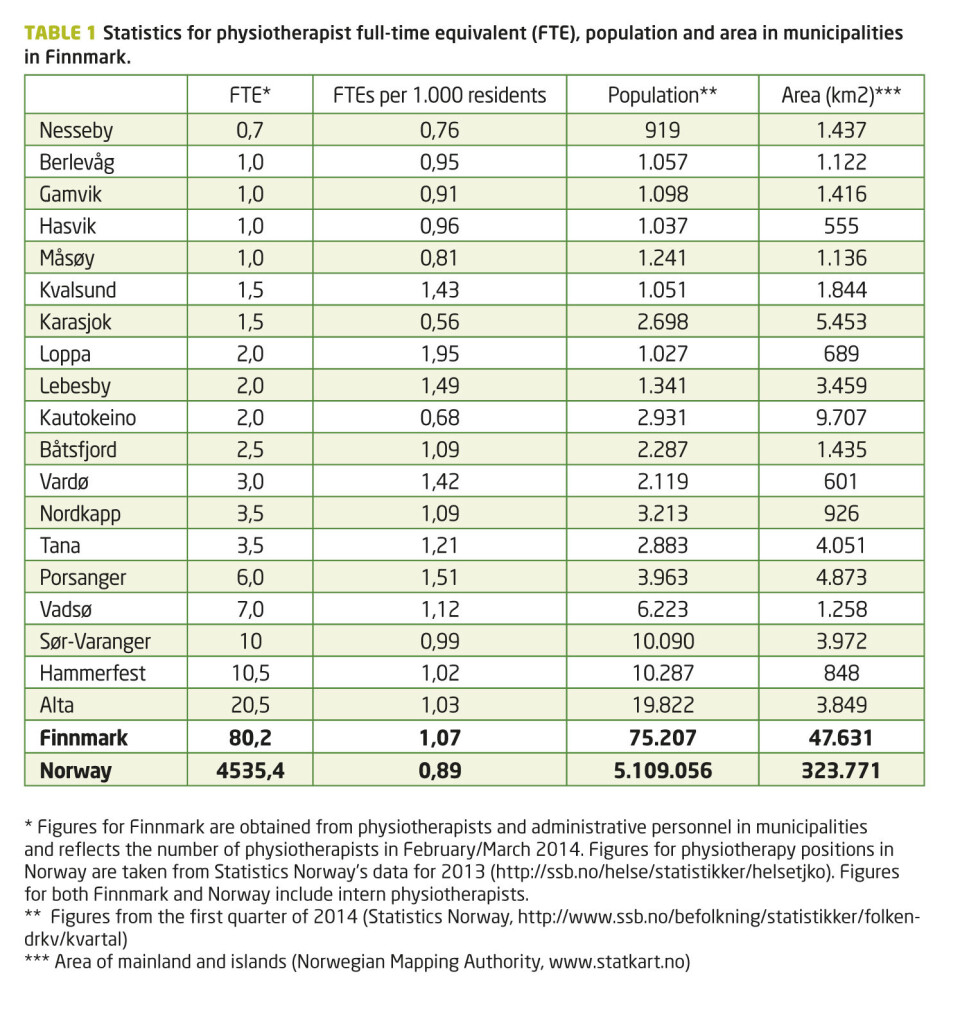
In Norway there’s a recognized political objective to provide everyone with equal access to physiotherapy services, no matter where in the country you live. Finnmark County constitutes 15 percent of Norway’s land area, but has only 1.5 percent of the total population (1,2). Compared to the rest of the country, the population in Finnmark’s municipalities isn’t particularly low, but there are long traveling distances and transportation challenges. Seven of the country’s ten biggest municipalities are in Finnmark County (1), so even though 75 percent of the county’s population live in cities or towns (3), great distances cause challenges in providing everyone with equal physiotherapy services. Additionally, many of the physiotherapists work with few or no colleagues (table 1) and must handle a multitude of different tasks.
Up until the Municipal Health Reform of 1984, physiotherapy in Norway was mainly a service provided by private practitioners to patients 17-69 years of age (4-6). With new legislation, all municipalities were required to cover physiotherapy service to all. To steer the practice in the right direction, operating grants were introduced for private practitioners and government grants were given to fund municipally employed physiotherapists (from here also referred to as «employed»). The goals were to give more people access to the services and to even out the geographical distribution of physiotherapists. Children, adults with physical disabilities and/or chronic disease, and intellectually disabled persons were given priority to physiotherapy services. The thought was that the employed physiotherapists were going to focus on cases that private practitioners had difficulties prioritizing (4-6).
With the Coordination Reform (7) the municipalities have gotten a more extensive responsibility for health care, but at the same time more freedom to organize the health services as they see fit. The legislation has changed in important ways for physiotherapists, like municipalities no longer being required to provide physiotherapy services (8). Simultaneously, the municipalities are expected to increase competence, capacity and quality in their health services (7, 9, 10). Key goals are to limit the development of disease and disability and reduce the need for costly specialist health services. Thus, the government wants the municipalities to focus on health promotion, prevention, rehabilitation and chronic care – fields where physiotherapists have relevant competence and can contribute to goal attainment. However, statistics show that physiotherapy resources haven’t increased in recent years (11), and the Norwegian Physiotherapist Association reports a lack of commitment and funding in key areas (12,13).
The research as of today indicates a need for further study on what kind of challenges physiotherapists in Finnmark and similar areas face (Footnote 1). Kaale’s thesis on Troms County from 1995 (4) is relevant, since it illustrates physiotherapists’ challenges in regard to role definitions and priorities. On the other hand, this study is twenty years old and deals only with employed physiotherapists. Furthermore, we have only found a few foreign studies dealing with similar themes (14-16).
Footnote 1: We have conducted literature searches in AMED, EMBASE, MEDLINE and PedRO, and have examined several official documents and reports
We have examined what views physiotherapists in Finnmark’s municipalities have on the relationship between the municipalities’ resources for physiotherapy, the inhabitants’ needs and their own priorities. This article poses the following research question: How do physiotherapists in Finnmark’s municipalities describe and reason for their priorities and distribution of responsibilities? The purpose has been to gain more knowledge about the contents and tradeoffs in physiotherapy. This knowledge can form the basis for both discussing the existing physiotherapy practice, and developing it further in line with society’s needs.
This project has its theoretical base in the theory of professions (17, 18). A view of physiotherapy as a professional activity allows for an understanding of how traditions and norms specific for physiotherapy characterize participants' judgments and choices. The ability to exercise discretion and prioritize is in this perspective considered an integral part of professional work. The theoretical base includes an eye for the importance of the practice’s institutional setting (organizational and economic conditions). The analysis process also utilized key ethical principles, like equality and individualization (19, 20).
Method
We chose to conduct focus group interviews because it is a suitable method to obtain information about people's experiences, opinions, understandings and needs. Interaction between participants stimulates discussions about how they relate to topics, deliberate and make decisions (21,22).
We conducted five focus group interviews with three to five participants in each interview (n=21) in January-March 2014. After obtaining a complete overview of municipally affiliated physiotherapists in Finnmark (municipally employed and private practicing with subsidies), we carried out a strategic recruitment among these. Employed physiotherapists were recruited by permission from their immediate leader, while private practitioners were contacted directly. Participants were first contacted by telephone, then in writing. The criterion for inclusion was a minimum of six months of work in the municipality.
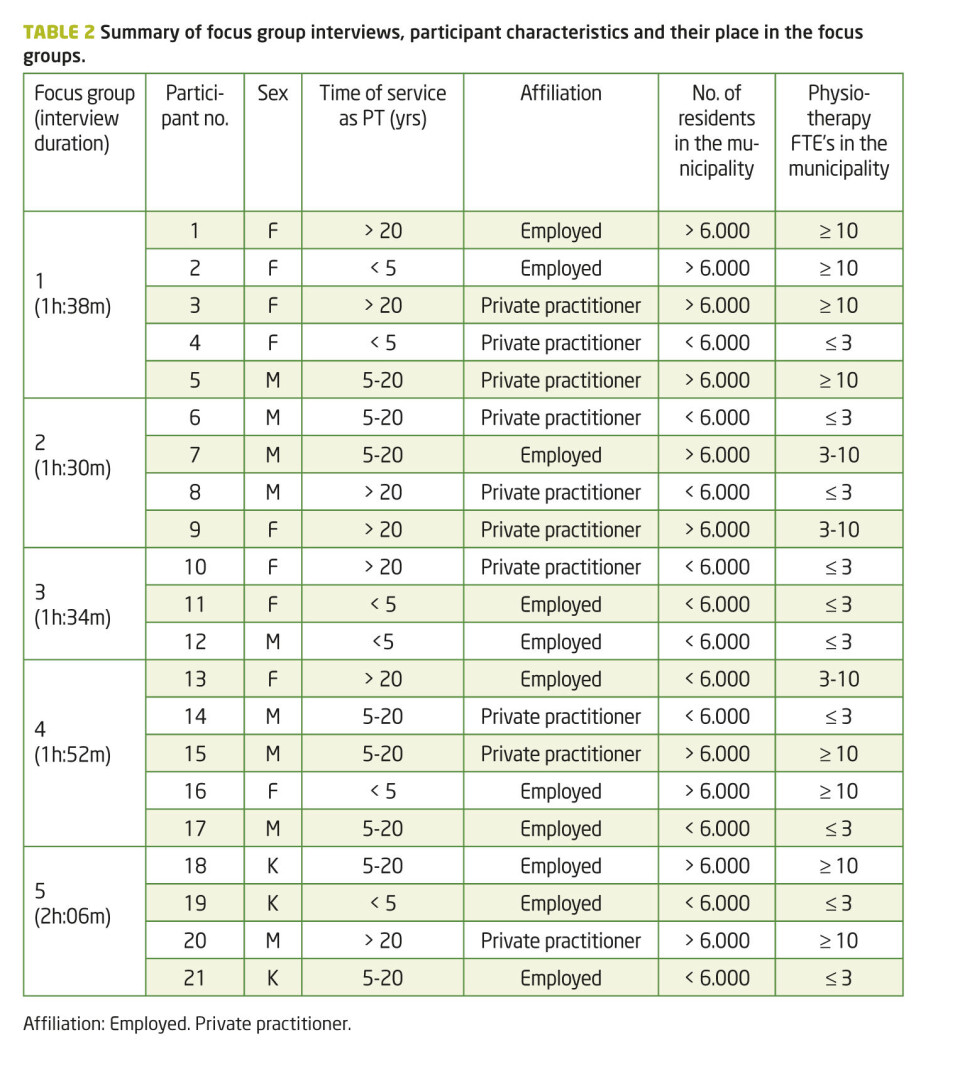
To bring out contrasts, the focus groups were assembled in variations of seniority, gender and affiliation (employed/private practicing). In each focus group, we also looked among the participants for a range in municipality size, population, and the number of physiotherapists in the municipality (table 2). Overarching themes in the interview guide were professional resources and needs, areas of expertise, and cooperation. First author (MN) worked alone as moderator in the first three interviews, while the last two were conducted with third author (SM). The interviews were recorded with a digital audio recorder, and took place at the municipally employed physiotherapists’ offices.
Before each interview we clarified the expectation of confidentiality regarding information that would come up and that we wanted the participants to speak as candidly as possible. The interviews were characterized by trust, openness and factuality. The participants allowed themselves to be engaged by the project’s theme and contributed their own experiences and views, which made the content of the interviews relevant and multifaceted.
First author listened to and transcribed the recordings verbatim. The data analysis began in parallel with continued collecting of data. The interview guide was adjusted continuously according to new insights from the interviews, but the overall theme was retained throughout the process. We conducted a thematic content analysis by alternating between what each participant had to say about specific themes, and taking cross-sectional looks at participants and interviews (22,23). Important themes emerged in the interaction between research questions, data and theory. We revised and fine-tuned the research questions during the analysis process. To ensure valid interpretations, all of the authors examined the interview material and discussed data collection, analysis, interpretation and written presentation.
All participants gave their written consent voluntarily before the interviews. Findings are presented in a manner that safeguards the participant's anonymity.
Findings
The participants thought that the municipal resources for physiotherapy did not correspond with their tasks and the inhabitants' needs. On this basis, the challenges related to prioritization and allocation of patients and tasks became the central theme in the focus group interviews.
Prioritizing is Left to Physiotherapists
All the physiotherapists, both employed and private practitioners, made it clear that tough choices on the basis of limited resources were largely left to them to decide. Only two of the 13 municipalities that were represented in the survey had formalized guidelines for prioritization.
When asked about balancing between patient groups, the participants often responded in general terms, but it emerged that the highest priority was children, patients that recently had undergone surgery, and patients with newly onset neurological conditions. All emphasized the importance of an assessment of needs and usefulness as a basis for ranking: Conditions that were acute, or would deteriorate quickly without follow-up, were given high priority, while «chronically ill patients» and «things that can wait» were prioritized as secondary. Many found themselves continually being forced to put on hold patients who needed follow-up, which they perceived as stressful.
Most of the physiotherapists did not participate in work that was primarily preventive and health promoting, but there were exceptions: In some municipalities, the employed physiotherapists performed routine checks on children, and a few ran preventive group programs for adults. None of the private practitioners reported participation in preventive work. The physiotherapists who did not participate in preventive work and health promotion nevertheless considered this work important and would like to contribute more in these fields. However, with the current resource situation and revenue model in the private sector, it would be infeasible to prioritize people who could get sick some time in the future over patients requiring follow-up then and there.
Patients who lived in remote areas and required home visits were in danger of not getting treatment. The dilemma was in choosing between spending a lot of time traveling to individual patients or to provide treatment to more people. One participant stated: «Of course, we have patients who require home visits, too. There we notice that some are simply not being prioritized because they live [remotely].»
Prioritization and Distribution
The size of the physiotherapists’ professional environment in the municipalities and their affiliations characterize prioritization and allocation of patients and other duties.
Specialized expertise was strongest in the municipalities with the most physiotherapists. Patients there were largely distributed based on professional competence, which helped to limit the framework for priorities that each physiotherapist had to make. Participants from the municipalities with the smallest professional environments took care of many different patient groups and activities, and thus had to do more complex tradeoffs. They portrayed a strong personal responsibility for the physiotherapy service, found the extensive competence requirements challenging, and missed being part of a larger physiotherapy environment. Both the private practitioners and those employed in municipalities with few physiotherapists clearly saw the shortcomings in the overall physiotherapy service, but simply couldn’t provide everything as well as they wanted. One employed participant, who was the only physiotherapist in the whole municipality, stated: «What I struggle with is to provide a good enough service to the chronically ill and children. There is an infinite amount of things one can do, but how do you choose? That’s the part I struggle with the most to… So my conscience doesn’t kill me.»
All the participants in this study appeared as conscientious professionals, but the private practitioners were consistently clearer on the boundaries of their responsibility. However, private practitioners in municipalities with small professional environments came off as more flexible than those in municipalities with larger professional environments.
Private practitioners in municipalities with the most physiotherapists were the participants who differentiated the strongest between the responsibilities of «municipal» and «private» physiotherapists. They were adamant that examination and treatment of patients in their physiotherapy clinics were the most important priorities and all other duties were considered in the light of whether they came at the expense of these priorities. Time spent on non-clinical tasks like gathering patient information or attending meetings were therefore minimized. The reasoning was that such prioritization gave good income, and at the same time many referred patients received follow-up. Those who had the opportunity to do so, let municipally employed physiotherapists handle tasks that they did not think fit into private practice. The following statement was characteristic:
«One has to consider waiting lists: How many [patients] actually want treatment? How should I utilize that time when the municipality can take care of it? And then economy plays its part. Had it been insanely well paid – then I would have gone to several more meetings. But when you earn neither more nor less, you can say ‘OK, then I’ll treat instead, and the [employed] can handle that part.’»
In municipalities with the most physiotherapists and the most pronounced division of duties between private and employed physiotherapist, the employed ones assumed special responsibilities for children, elderly patients and patients in municipal institutions (e.g. nursing homes). All participants who worked in municipalities with both private practitioners and employed physiotherapists agreed that patients who were «difficult» or «complex» were «a municipal responsibility», since the employed could use their work time more flexibly and without regard to income.
Different Framework and Different Focus
The participants’ affiliation as private practitioners or employed seemed to be of significance considering the tasks they perceived as important. A participant running a private practice in a municipality with few inhabitants characterized himself as a «jack-of-all-trades» because his workday demanded versatility, but said: «I am curative, though. That’s my main job.» Statements like this was repeated by participants from private practices, including those who had a broad practice and participated in many different areas.
Some municipalities had strengthened the service with a permanently employed physiotherapist during recent years. Private practitioners in such municipalities admitted relief not to have to fulfill requirements of certain patient groups:
«I don’t have to deal with nursing homes, stroke patients, dementia patients, and things like that anymore. It might be that [the employed] have three to five patients every day, and have the time to take care of those stroke patients in a completely different way than I do. ‘Cause when you have the timesheet [that I do] things move very quickly, you know?»
In contrast to this were employed physiotherapists who noticed an influx of «outpatient» and «curative» patients, but wanted to prioritize others, for example patients in nursing homes and patients in need of multidisciplinary rehabilitation.
Purchase of Services
Several municipalities with only private practitioners had made agreements for the purchase of services not covered by the tariff regulations (i.e. the revenue model for private practitioners, part of social security). One municipality paid a private practicing physiotherapist to work three hours a week at a nursing home. This physiotherapist stated:
«That’s nothing. Stuff like that is just putting out fires. And when you get patients transferred from the hospital, like people having had hip surgery, then a lot of your time is spent on them that week. And the next week you can treat the residents, since there are no critical cases. After that, maybe you’ll get a stroke patient, and you might have to spend four weeks treating only that patient.»
A different municipality with only private practitioners purchased up to seven hours each week, but neither there did the physiotherapist think it was possible to do all tasks satisfactorily. Unlike most other participants (both private practicing and employed) from municipalities with few physiotherapists, this physiotherapist delineated the personal responsibility by making the municipal administration jointly responsible for priorities:
«There are certain groups that do not get anything, that have been requested. Like focusing on schools, to do follow-up there. (…) But again, in cooperation with the administration, the head of health and care services, what they want. Because, like I said: I do what they want me to do.»
Duties of Employed Physiotherapists are in Transition
Employed physiotherapists were required to do non-clinical tasks, such as working with care plans for individuals in need of long-time follow-up («Individuell Plan»), to do other service coordination, and management of assistive aids. For some, this took a lot of time away from their other tasks, and many were frustrated that it happened at the expense of what they perceived as their core duties: examination and treatment, health promotion and preventive care.
Unlike the private practitioners, the employed physiotherapists described their duties as in transition. Constantly, new tasks had to be managed, particularly in priority areas such as rehabilitation and prevention. Several participants stated that they dreaded getting additional responsibilities without an increase in capacity, since the amount of other work was not reduced. Many employed physiotherapists thought that they, as a result of this, distributed their resources on too many patients, and the phrase «spread too thin» appeared in several interviews. The private practitioners, however, stated that they did not spread their resources too thin, but rather gave individual patients adequate follow-up and let others wait. While the employed group expressed frustration over insufficient time for each patient, the private practitioners were exasperated by long waiting lists.
In one municipality, the employed physiotherapists had constructed a system for managing deviations to avoid «spreading too thin.» The system involved the registration of patients who didn’t receive follow-up within a deadline. It helped the physiotherapists be more aware of the tradeoffs and see what they didn’t have time to take care of: «We felt we did a poor job with the patients. We decided that we have to complete and finish, and give patients what they actually need. And then we’ll just highlight that we can’t manage to do it [all].»
Discussion
Differences in priorities between private and employed physiotherapists must be seen in context of both professional traditions, the physiotherapy service's historical development in municipalities, and existing practice frameworks. The focus group interviews show that there is a close link between the participants' priorities and their professional identity as either private practitioners or employed. The traditional differences are reflected the strongest in municipalities with the most physiotherapists (more than three), in the form of clearly defined division of tasks, while they are less pronounced in the municipalities where each physiotherapist must concentrate on numerous issues.
Fixed frameworks
Problems covering the spectrum of different tasks are most apparent in municipalities with only private practicing physiotherapists, since the income structure for private practice provides both guidance on choices and legitimizes clear boundaries for responsibility. Today's tariff regulations admittedly also reward other tasks than examination and treatment: activities such as traveling, home treatment and participation in meetings entitle payment. Other tasks are not covered, including treating patients in institutions, administrative duties, preventive care/health promotion, attendance at public health centers and in school health services (24, 25).
Municipalities may require that up to 20 percent of the private practitioners' contracted time is directed toward «unmet needs», but this only applies to activities mentioned in the tariff regulation (26). Therefore, municipalities must enter special agreements for the purchase of services if private practitioners are to conduct other tasks. The interviews showed that such agreements with strict time limitations may cause insufficient patient follow-up, e.g. in nursing homes. In these cases the restricted framework might lead to prioritizations that conflict with the physiotherapists’ professional opinion of what is right to spend available time on.
Individualizing Responsibility
The fact that physiotherapists think that municipal resources are inadequate is not a new perception (4, 27). Allocated resources for health care will always be limited, and prioritization on the basis of discretion is part of a health professional’s job (17). The participants' descriptions of capacity still makes it appropriate to question whether current resources are in reasonable proportion to the tasks and ambitions.
What constitutes adequate physiotherapy resources in a municipality depends on what the physiotherapists’ tasks and responsibilities should be. The interviews show that this is not always clearly defined. Part of what makes the physiotherapists' work in municipalities demanding is that the same professional can potentially have many different tasks. Physiotherapy in municipalities currently includes not only curative treatment, but also chronic care, re-/habilitation, preventive care and health promotion. Kaale’s (4) proposal to consider prioritization dilemmas in physiotherapy not only on the basis of lack of time, but also in light of conflict regarding the professional content of physiotherapy, still seems relevant: Available time must be seen in relation to the tasks that the authorities as well as the physiotherapists themselves expect physiotherapists to take care of.
An important question is where to draw the line between the physiotherapist’s and municipality’s responsibility. As professional service providers in a welfare state, physiotherapists have professional autonomy, responsibility for proper professional practice and the mandate to make discretional priorities (18). But the responsibility for implementing centrally agreed health priorities cannot be placed solely on the shoulders of individual physiotherapists. Municipalities are responsible for organizing the service in such a way that physiotherapists can make priorities without compromising their professional integrity or be held personally accountable if the services are inadequate due to capacity issues. When difficult choices caused by limited resources are left solely to physiotherapists to handle, with little involvement from local authorities, the responsibility is being individualized.
In 1997, the Lønning Committee II (28) clarified the distinction between two priority levels: First-order prioritization decisions are taken at a superior system level, and concerns what kind of services one should offer and how extensive they should be. Second-order prioritization decisions concerns specific decisions about individuals, such as who should get access to existing services. The physiotherapists’ responsibility is primarily the latter, but the levels are also linked: The priorities municipalities make by scaling the service, deciding tasks and determining affiliation, sets the framework for the physiotherapists’ practice and professional autonomy. Therefore, this has consequences for the service offered to inhabitants.
Municipal Accountability
Today it is expected that health care professionals should contribute to health promotion and disease prevention, and not just have an eye for the needs of the individual patient. Simultaneously, the responsibility for disadvantaged and vulnerable people is a fundamental and universal moral principle that characterizes the work of health professionals (20). The physiotherapists in our focus groups had difficulties prioritizing the «new» tasks that the government wants municipalities to pursue, and expressed considerable frustration over the disparity between political and professional ambitions and the realities. The physiotherapists thought, for example, that prevention was important and relevant work for physiotherapists, and were aware of the health policy guidelines. But professional tradition, ethics and economic considerations indicated that other responsibilities came first.
Distribution of scarce resources can lead the principles of individualization and equal treatment into conflict. As for which one is more important – the individual patient's specific needs or equal treatment of patients in relation to each other – there is no unambiguous and morally correct answer; achieving a good balance between the two requires exercise of discretion. Nalette (19) writes, on the basis of virtue ethics, that physiotherapists’ primary moral responsibility and ideal is to help the individual patient. The argument is that the disadvantages with some patients having to wait or being omitted, are cancelled out by the benefits of others receiving adequate follow-up, while physiotherapists can live up to their professional standards and preserve their integrity. Tight frames can over time cause adverse changes of practices, such as the development of a cultural acceptance to give patients insufficient follow-up. If, instead, physiotherapists lead well-founded and visible priority practices that do not hide a lack of resources, then this can lead to highlighting the dilemmas and choices. It can also help provide necessary feedback about the consequences of underfunding, and place the ultimate responsibility for services with the management of the organization (19).
The Validity of the Findings
In qualitative research, findings are made applicable through analytical generalization (29). Strategic selection of participants makes it likely that patterns in the data represent categories that are valid also in similar contexts. We believe that our findings and interpretations can be generalized to other small and medium-sized municipalities in Norway, and to the challenges physiotherapists face there.
Conclusion
The study shows that physiotherapists in municipalities in Finnmark consider the allocated resources to physiotherapy not to match the needs of the inhabitants and the politicians’ ambitions for the health services. The physiotherapists expressed that they themselves must handle the prioritization dilemmas that arise, without much support from the municipalities. The analysis suggests that variations in capacity, affiliation and priorities, as well as having to travel long distances, lead to uneven physiotherapy services based on place of residency. This is not in line with health policy goals of equitable health care for all.
The findings highlight the importance of the municipalities scaling the physiotherapy services sufficiently, collaborating with the physiotherapists on priorities, and arranging for all prioritized tasks to be taken care of. The municipalities’ responsibility includes making informed decisions about which form of affiliation is appropriate; whether they should employ their own physiotherapists or recruit private practitioners. The balancing act between municipal control and professional autonomy is a dilemma that may be important to investigate further.
Acknowledgments
The research project is funded by The Norwegian Fund for Post-Graduate Training in Physiotherapy and Northern Norway Regional Health Authority (Helse Nord RHF).
References
1. Kartverket. Arealstatistikk for Norge: http://www.statkart.no/Kunnskap/Fakta-om-Norge/Arealstatistikk/Oversikt/.
2. Statistisk sentralbyrå. Folkemengd og befolkningsendringar: http://ssb.no/befolkning/statistikker/folkendrkv.
3. Statistisk sentralbyrå. Befolkning og areal i tettsteder: http://ssb.no/befolkning/statistikker/beftett-
4. Kaale HK. Kommunefysioterapeutrolla – korleis den er og korleis den blir forma. Hovedfagsoppgave. Tromsø: Universitetet i Tromsø, 1995.
5. Kaale HK, Hauksdottir N. Fysioterapi under kommunehelsereforma – 20 år etter. Fysioterapeuten 2002; 69(14): 20-4.
6. Sosial- og helsedirektoratet. Kartlegging av fysioterapitjenesten i kommunene. For perioden 1984-2005. Oslo: Sosial- og helsedirektoratet, 2007.
7. Helse- og omsorgsdepartementet. Stortingsmelding 47 (2008-2009). Samhandlingsreformen: rett behandling – på rett sted – til rett tid. Oslo: Helse- og omsorgsdepartementet, 2009.
8. Lov om kommunale helse- og omsorgstjenester m.m. (helse- og omsorgstjenesteloven), 24.6 nr. 6 2011.
9. Helse- og omsorgsdepartementet. Innovasjon i omsorg. NOU 2011: 11. Oslo: Departementenes servicesenter, Informasjonsforvaltning, 2011.
10.Stortingsmelding 16 (2010-2011). Nasjonal helse- og omsorgsplan (2011-2015).
11.Statistisk sentralbyrå. Kommunehelsetenesta, årleg: http://ssb.no/helse/statistikker/helsetjko.
12.Lindvåg D. Kommunene satser ikke på fysioterapi. Fysioterapeuten 2013; 80(8): 15.
13.Engseth E. Tallenes tale. Fysioterapeuten 2012; 79(7): 43.
14.Gunn H, Goding L. Continuing Professional Development of physiotherapists based in community primary care trusts. Physiotherapy 2009; 95: 210-5.
15.Jin C, Ishikawa A, Sengoku Y, et al. A telehealth project for supporting an isolated physiotherapist in a rural community of Hokkaido. Journal of telemedicine and telecare 2000; 2: 35-7.
16.Sheppard L. Work practices of rural and remote physiotherapists. The Australian journal of rural health 2001; 9: 84-90.
17.Grimen H, Molander A. Profesjon og skjønn. I: Molander A, Terum LI, red. Profesjonsstudier. Oslo: Universitetsforlaget, 2008: 179-96.
18.Molander A, Terum LI. Profesjonsstudier – en introduksjon. I: Molander A, Terum LI, red. Profesjonsstudier. Oslo: Universitetsforlaget, 2008: 13-27.
19.Nalette E. Constrained physical therapist practice: an ethical case analysis of recommending discharge placement from the acute care setting. Physical therapy 2010; 90: 939-52.
20.Wifstad Å. Helsefagenes etikk: en innføring. Oslo: Universitetsforlaget, 2013.
21.Barbour R. Doing focus groups. London: SAGE, 2007.
22.Wibeck V. Med fokus på interaksjon. I: Fangen K, Sellerberg A-M, red. Mange ulike metoder. Oslo: Gyldendal, 2011: 15-36.
23.Thagaard T. Systematikk og innlevelse: en innføring i kvalitativ metode. Bergen: Fagbokforlaget, 2009.
24.NAV. Fastlønnstilskudd til fysioterapitjenesten i kommunene, rundskriv: https://www.nav.no/rettskildene/Rundskriv/147835.cms
25.Forskrift om stønad til fysioterapi m.m., 25.6 nr. 8 2014.
26.KS' kommunetarutgave til ASA 4313 for perioden 2013-2014: http://ks.no/tema/Arbeidsgiver/Lov-og-avtaleverk/Fysioterapiavtaler/Kommentarutgave-til-rammeavtalen-ASA-4313/
27.Agenda utredning & utvikling AS/Helse- og omsorgsdepartementet. Spørreundersøkelse om fysioterapi i kommunehelsetjenesten. Høvik: Agenda utredning & utvikling AS, 2009. http://www.regjeringen.no/upload/HOD/Dokumenter%20KTA/R6302%20HOD%20Fysioterapeuter%20250209.pdf
28.Sosial- og helsedepartementet. Prioritering på ny: gjennomgang av retningslinjer for prioriteringer innen norsk helsetjeneste. NOU 1997: 18. Oslo: Statens forvaltningstjeneste, 1997.
29.Kvale S, Brinkmann S. Det kvalitative forskningsintervju. Oslo: Gyldendal akademisk, 2009.























